Ambulatory phlebectomy is a surgical procedure for removal of bulging varicose veins, carried out in an outpatient setting. It is usually performed in conjunction with an endovenous ablation procedure to eliminate an underlying source of venous hypertension. The varicose veins are mapped visually with the patient standing, using an indelible marker. The patient is then placed on the operating table and a more precise map is generated with a transillumination tool, the Veinlite. This preop mapping is important because tilting the operating table with the head down during the ablation causes the veins to collapse, making visualization more difficult. Local “tumescent” anesthesia is a dilute solution of lidocaine and epinephrine in saline. It can be used to anesthetize large areas without a toxic effect. The epinephrine reduces bleeding and prolongs the anesthetic effect of the lidocaine. Unless the patient has a phobia for needles or is extremely nervous about the procedure, oral sedatives are not needed.
Illustrations courtesy of Dr. Jose Almeida
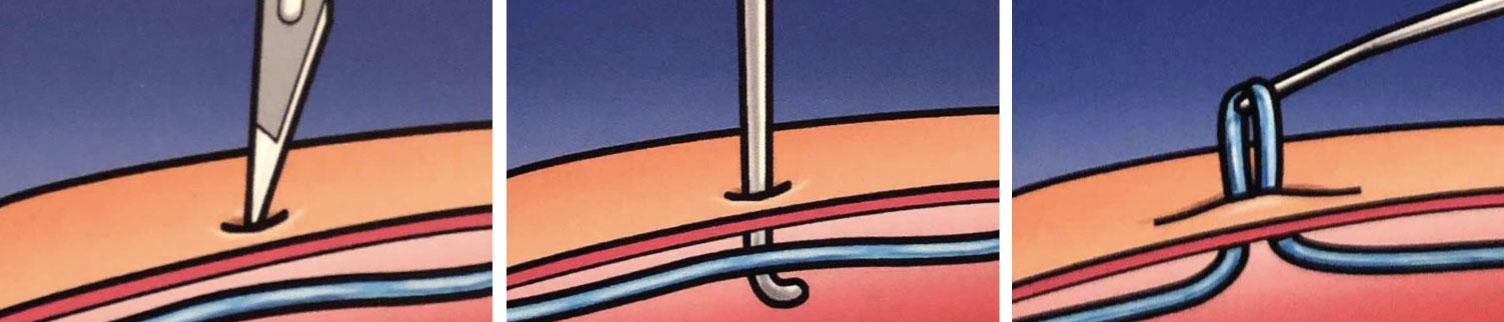
The varicose veins are accessed through 1-2 mm incisions, through which the veins are extracted, using a tiny hook.

The varicose veins are accessed through 1-2 mm incisions, through which the veins are extracted, using a tiny hook. The loop of vein is then pulled with fine hemostat clamps with gentle traction, until it breaks. The two cut ends of the vein then retract under the skin. There should be minimal blood in the vein because most of it drains when the table is angled with the head down. The epinephrine also helps minimize bleeding. I prefer to make round incisions with a 1 mm punch. These remain open longer than linear incisions. A compression stocking is applied, gauze pads are placed over the phlebectomy sites, and these are held in place with tightly wrapped Ace bandage. The stocking and gauze bandages are applied while the patient’s head is down, so blood is prevented from flowing back into the veins when the patient stands. This steady compression “squeezes" blood deep to the incisions out through the holes and into the gauze. This greatly reduces bruising and post-procedure pain. The patient wears the stocking and dressings for 2-3 days, after which they are removed. Patients are advised to avoid hot baths and high intensity leg exercises for 1 week, after which there are no restrictions. The wounds are checked after 2 weeks, or sooner if the phlebectomy was performed with an ablation. Narcotic analgesics are almost never required, and only 10% of our patients use an NSAID for pain relief.

Before (Left), After (Right)

